The Matron’s Medical Report Book is the earliest surviving record we have from Stannington Sanatorium, which contains monthly updates on patient progress and general administration. The first entry from the Report Book, below, dates from 1908 and lists some of the earliest patients with details of their ages, addresses and condition whilst in the Sanatorium.
April 11th 1908
“There are now six patients here. Five have been here for nearly four weeks (since March 18th) & one for three weeks. They are:-
1. Maggie Smith, aged 17. Address 73 Leopold St (sent from the Gateshead Workhouse)
2. John Edward Kenney, aged 15 ¾; Address 72 William St, Hebburn Quay (working at Hebburn Colliery)
3. James Robson, aged 13. Address 16 Bottle Bank, South Shields
4. Thomas Hill, aged 12 ½. Address 76 Belvedere St, Heaton
5. John Nicholson, aged 10. Address 10 Hyiamais Court, Gateshead
6. Thomas Burns, aged 16 ¾. Admitted March 21st. Address 40 Stanley St, Jarrow
The general condition of all the patients has considerably improved. They have all gained in weight during the last 18 days: Maggie Smith 5 ¼ lb, John Kennedy 4lb, James Robson 2 ¾ lb, T. Hill 3lb, J. Nicholson 3 ¾ lb, T. Burns 3 ¼ lb (all given to the nearest ¼ lb). Only one patient, Maggie Smith, has any marked degree of fever. There is a slight improvement in her temperature. One patient, J. Hill, does not cough at all. All the others are coughing less and bringing up less sputum.
Examination of the sputum for tubercle bacilli has not yet been possible.
The local condition in three patients, T. Burns, T. Hill & J. Nicholson is quite satisfactory, shewing improvement. In two patients, Maggie Smith & J. Robson it has remained about the same.
In one, J. Kennedy, there has been some extension of the diseased area, but improvement again during the last four days after strict rest.”
[HOSP/STAN/2/1/1]
The close association of tuberculosis with poor living conditions is further highlighted here by the first two patients who have come from Gateshead Workhouse and Hebburn Colliery respectively. At this stage there were only 6 patients but the sanatorium had opened not long before this with provision for 40 children and soon saw the beds fill up. In the following years the sanatorium’s capacity began to expand rapidly with an extension providing an additional 50 beds opening in 1911 and several new wards opening in the 1920s so that by 1926 there were 312 beds available.
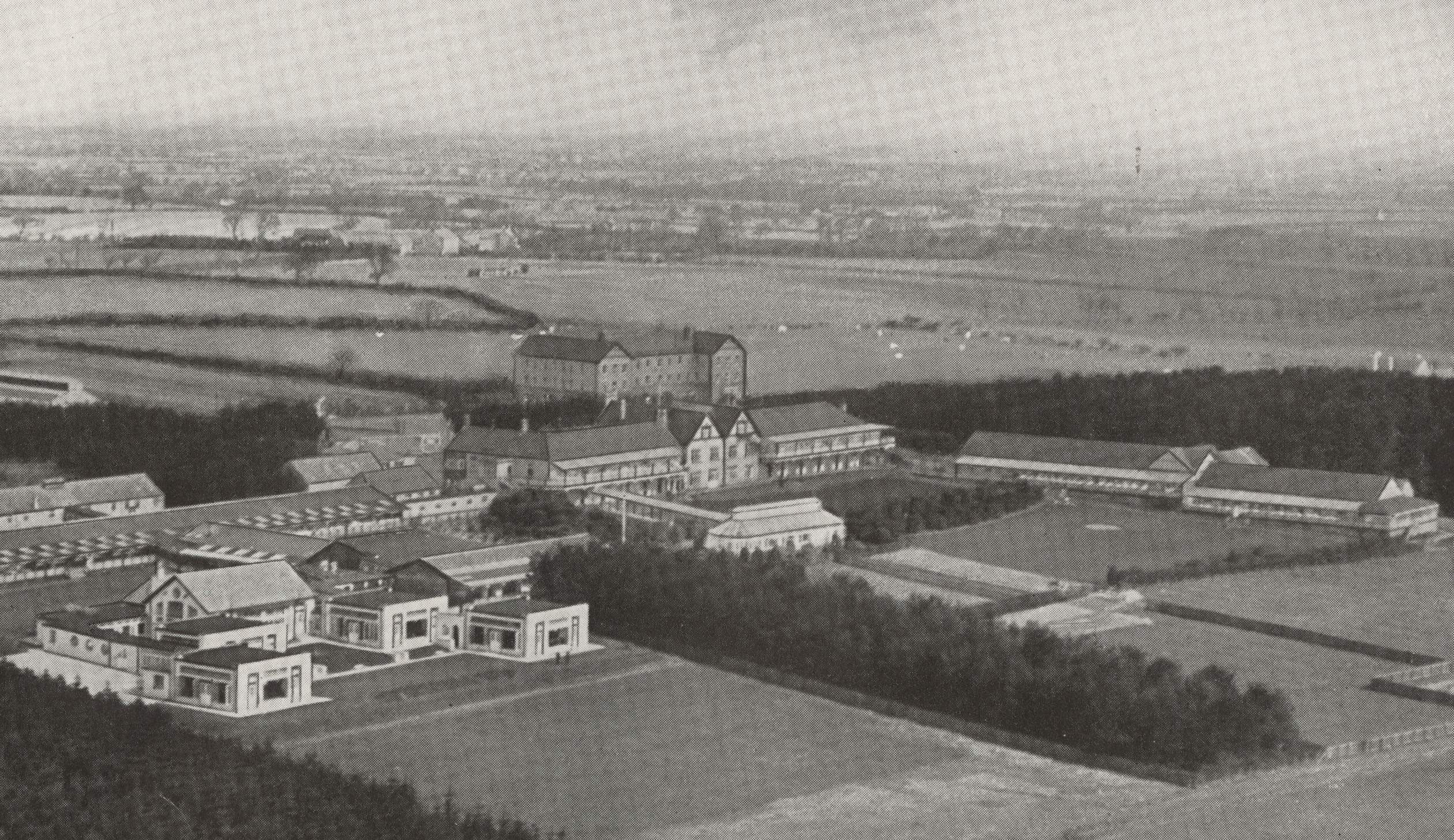
Aerial view of the sanatorium c.1936
[HOSP/STAN/9/1/1]
We will post some more entries from the Matron’s Report Book in future blog posts to track the progress of the early days of the Sanatorium.