Amongst the 2242 sets of patient radiographs we hold there are 55 for which we do not have any corresponding patient case notes. Within this group of 55 there is one patient in particular that stands out as the radiographs that survive for him are the earliest original radiographs we hold with the others all being on microfiche. The other 54 also have their patient numbers clearly marked on the radiographs and references to them can be found amongst the other records in the collection, for example admission registers and treatment registers.
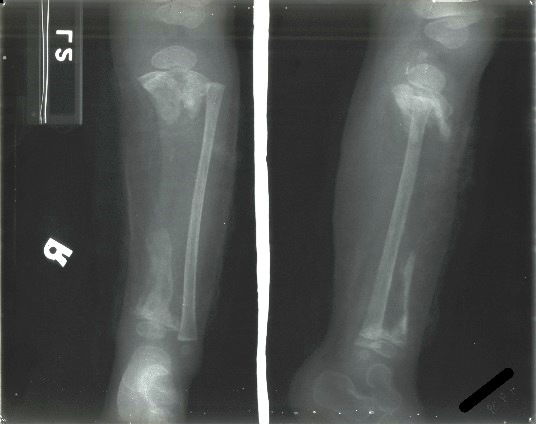
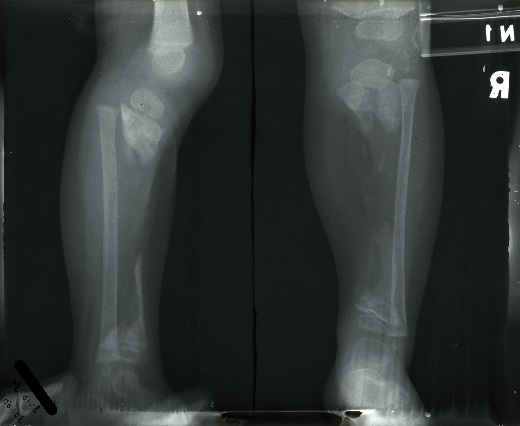
All we know about this patient is his name and the date on which the x-rays were taken. The three x-rays were taken in September and October of 1939 and show the boy’s right arm and right leg. Judging from his size we are assuming he was relatively young and was evidently suffering from disease of the right tibia and right forearm. There are no later re-admissions for this patient and so we are assuming that he either recovered and was discharged with no later relapse or that he died. We have the sanatorium school records for the period as well and there is no mention of him there, so again we can assume he was either below school age or too ill to attend. The only other contemporary records we have where we might expect to find him are the register of operations and the register of splints and appliances. Again there is no reference in either of these confirming he did not receive any surgical treatment during his stay and was not issued with a splint.
 Click on the images to enlarge
Click on the images to enlarge
If you can offer any additional details about this patient from his radiographs please add them to the comments below.
X rays of a child which based on visible ossification centres of the wrist approx 2 years old . X-rays of the right tibia and fibula show extensive areas of osteolysis throughout the tibial diaphysis. Fibula is preserved by comparison. X rays of the right arm show large area of osteolysis in the distal radius metadiaphysis. Diagnosis of TB osteomyelitis but Tb in the bone can look like any other cause of bone destruction eg. tumour, non tb infection. Patient obviously infected for a long time without effective antimicrobial treatment to get this degree of destruction.
The incidence of skeletal manifestation in tuberculosis is very low, any bone can be affected, however spine is the most common site for skeletal TB, accounting more than 50% of all cases followed by femur, tibia and fibula. Tuberculous osteomyelitis is secondary to lymphohaematogenous spread with lung being the primary focus in 75% of cases5. Osteoarticular tuberculous is a rare form of disease accounting for 1-5% of all cases. Large weight bearing joints, long bones, skull and soft tissues can be involved. Primary diaphyseal TB of long bone is extremely rare and only few cases have been reported in literature. Clinical symptoms may be mild and the diagnosis of tuberculous osteomyelitis requires a high degree of suspicion for accurate and timely diagnosis.
Hello. It seems to me that this may be some kind of tumor. Probably giant cell tumor?!
The development of the tibia is in keeping with a child of approximately one year of age (Keats, Theodore E.; Smith, Thomas H. Atlas of Normal Developmental Roentgen Anatomy). Although it has been shown, using studies Greulich and Pyle’s Radiographic Atlas of Skeletal Development of the Hand and Wrist that skeletal, that development hasn’t changed significantly in the last decades we need to keep in mind that during serious illness bone maturation may lag behind.
There is clear osteolysis of both the tibia and the radius which spares the epiphysis. In contrast to the tibia the radius shows some callus formation (on the ulnar side).
It doesn’t look like a malignant bone tumor; the geographic distribution is rare as most bone tumors are solitary. In osteosarcoma one would expect at least bone formation and Ewing Sarc would have shown periostal reaction (specifically in the radius which is less involved). I don’t think that this is Giant Cell tumor. As that has the characteristic feature of going ‘to the end of bone’, i.e. in such extensive disease it would certainly involve the epiphysis.
The only bone tumor that I can think of that could cause such destruction would be Langerhans Cell Histiocytosis, which is a lytic multifocal bone tumor, but for LCH to lead to a disease in such an extend would be rare (at least nowadays).
But it is important to remember that bone tumors, in general and especially at such a young age, are extremely rare.
I agree with R. Robinson’s diagnosis. In contrast to the adult situation, in young children the epiphysis has its own nutrient vessels. After 12 to 18 months of age, these transphysial vessels disappear. As a result the physis acts as a natural border and prevents the spread of osteomyelitis from the metaphysis to the epiphysis. Most likely the imaging findings are the result of advanced osteomyelitis. Given the extend of disease this child certainly must have had severe complaints and cannot have walked on this leg. I don’t think that radiology will be able to tell which organism caused this.
Indeed an interesting and rare case! At the first sight (arm pictures) I thought of an osteogenesis imperfecta because of the periostal reaction, but the pictures of the legs do not seem to indicate such a diagnosis. I agree with Dr.Carnim’s suggestion: an osteolytic tumor, perhaps som kind of a giant cell tumor? I do not believe in an advanced osteomyelitis, which impossibly could reach to such an extent at that age of the patient. And hardly a TB as the epiphyses and not the diaphyses are the better preserved part of the bone.
I think there are 2 different pathological lesions
The right crural region; chronic osteomyelitis secondary to the trauma.
The right distal radius; malign tumor, probably Ewing sarcoma.