The spine is the most frequent site of skeletal involvement in tuberculosis of the bones and joints. Commonly known as Pott’s Disease, after Sir Percival Pott who first described the condition in 1779, tuberculous osteomyelitis of the spine affects between 25 and 60% of all individuals suffering from skeletal tuberculosis. It is most commonly seen in children and young adults, predominantly affecting the thoracic and upper lumbar regions of the spine, although evidence of cervical involvement also exists. Spinal lesions begin in the cartilage between the vertebrae or in one or more vertebral bodies, this leads to a narrowing of the joint space, noticeable in radiological examination. Paravertebral abscesses can also occur when diseased tissue in the vicinity of the affected vertebrae forms a mass and pus collects. With the expansion of this abscess there can be a loss of blood supply to the vertebral body resulting in a loss of integrity causing the vertebral column to collapse creating an angulation or ‘kyphosis’ to the spine. The collapsed vertebrae form a wedge, known as a ‘Gibbus deformity’, which can lead to compression of the spinal cord resulting in paraplegia, as well as functional problems with the pulmonary system.
There are numerous cases of spinal tuberculosis in the records from Stannington, all varying in their severity and final outcome. Below are two examples of the different types of spinal tuberculosis and the methods used to treat it.
Case Study 1 – Dorsal (Thoracic) Spine
Patient 17/1949, a 4 year old boy, was transferred to Stannington Sanatorium from the Royal Victoria Infirmary (RVI) in January 1949. His medical history had included a bout of pertussis, whooping cough, complicated by pneumonia followed a year later by lethargy and a swollen knee. In April 1947 he was admitted to Earl’s House Sanatorium with a primary tuberculous complex in the left upper zone of his chest and TB of the left upper tibial epiphysis and upper dorsal (thoracic) spine.
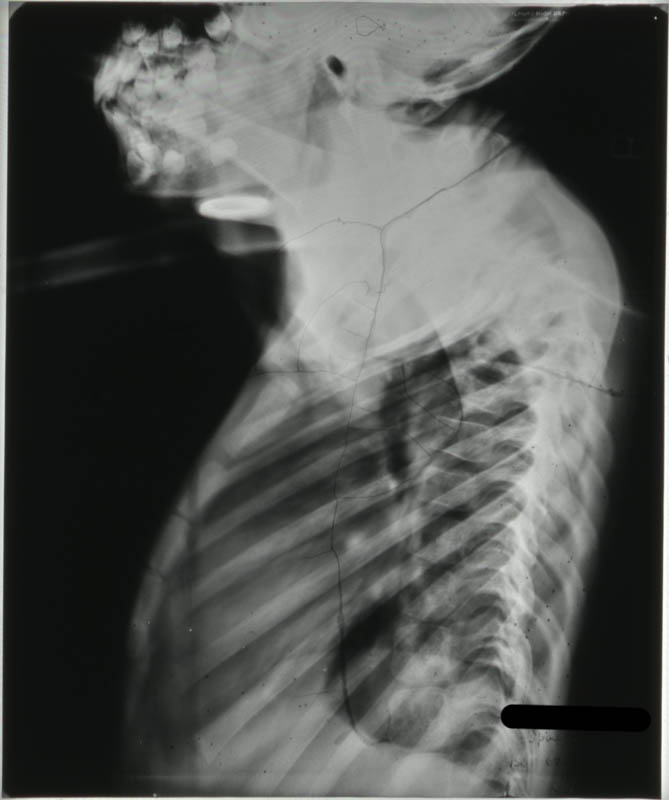
Paraplegia developed in September 1948 and he was transferred to the RVI that December showing signs of wasting and obvious kyphosis in the upper dorsal spine with paraplegia evident and total incontinence. His notes state that his head and thorax were encased in plaster cast, as was the left leg, to immobilise the affected areas. The incontinence was dealt with by applying a tube. Tuberculosis of the spine was relatively advanced, with the 3rd and 4th dorsal vertebrae having collapsed resulting in a noticeable kyphosis, seen in Figure 1.
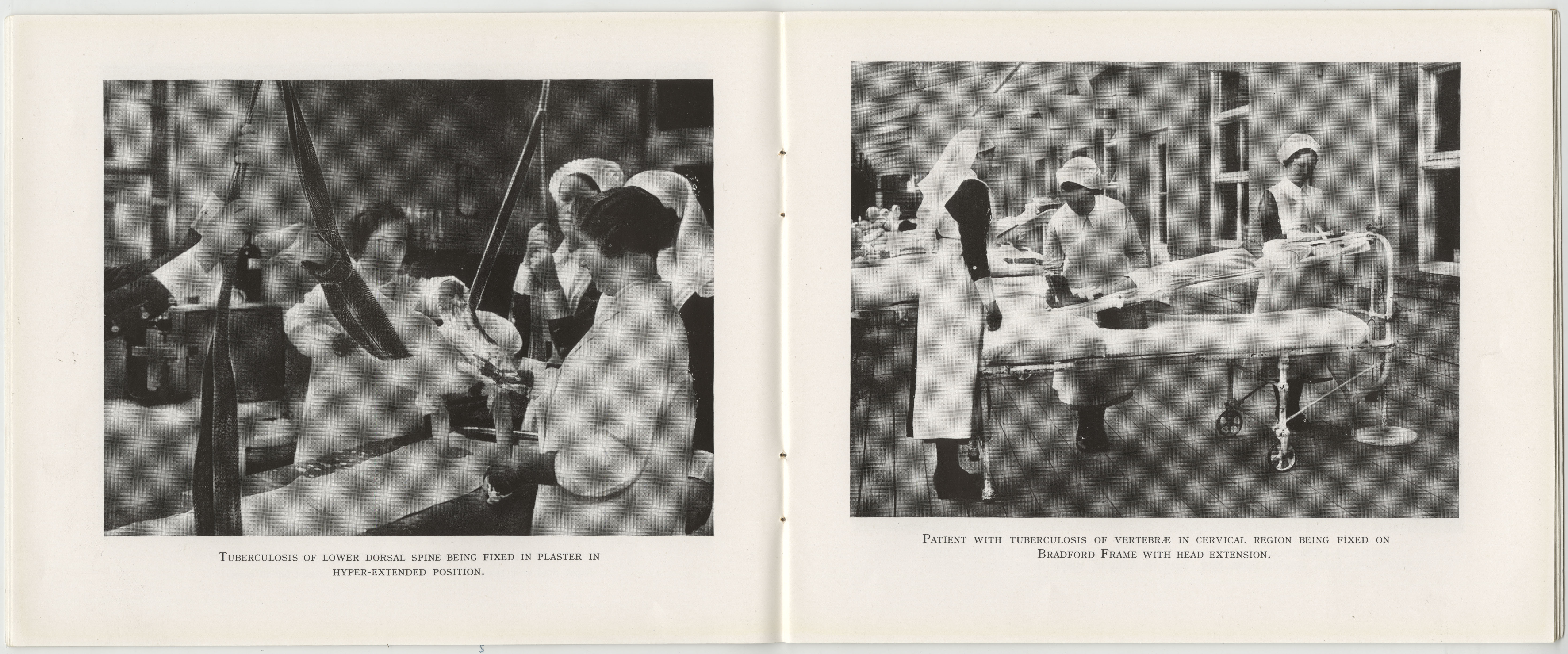
On admission to Stannington it is recorded that the radiographs showed a high dorsal lesion. The plaster cast encasing the head and thorax was removed and the patient was fixed to a short plaster boat with head piece, see left image in Figure 4.
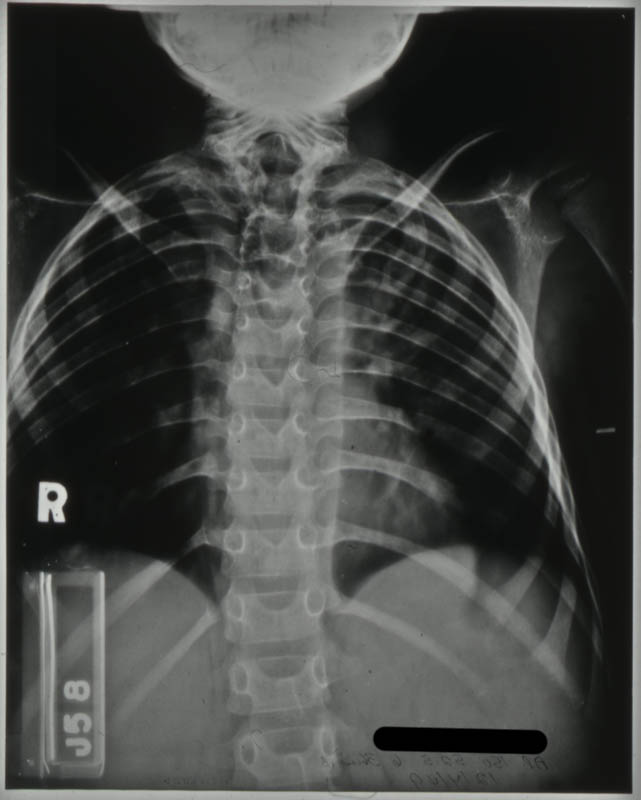

Radiographic images show further kyphosis, Figure 2, and the collapse of the vertebral bodies. Porosity is evident in the vertebral bodies in the upper dorsal region, identifiable by their translucent nature in Figure 3, giving rise to the extent of the infection.
In November 1949, the patient was fitted for a plastic splint. This was to fit
‘from the hips up the trunk extending over the neck to the occiput, reinforced with metal where necessary’.
The spinal lesion was considered quiescent by April 1952, all evidence of paraplegia having cleared up. However, he was to be fitted with a splint with a shaped head piece to immobilise the spine as much as possible. This patient was discharged in March 1953 and his brace discarded entirely in May 1953. He continued to be seen as an outpatient until February 1959.
Case Study 2 – Cervical Vertebrae
Patient 148/1948, a 3 year old girl, was initially admitted in January 1948 (Patient Number 8/1948) with a Primary Tuberculous Complex of the right mid-zone.
Preliminary medical reports described this girl as having had an enlarged right hilar shadow, a shadow of the hilar lymph nodes, and ‘shotty,’ swollen, glands with an impetigious lesion on the scalp. However, her initial stay at Stannington was short as she was removed against medical advice by her mother 28 days after admittance, only to be re-admitted seven months later with TB of the cervical spine.
Following an examination by the surgeon, Mr Stanger, on re-admission a comprehensive outline of her condition was given:
‘The lower surface of the 2nd c.v (cervical vertebrae) is involved; the body of the 3rd c.v is completely destroyed and the upper surface of the 4th is probably eroded.
This child should have every bone in her body x-rayed.’
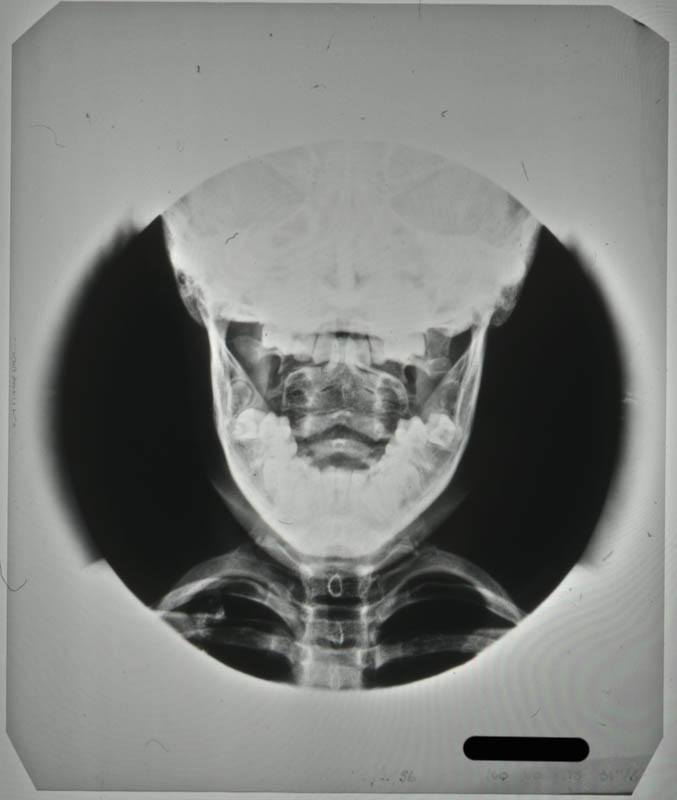
The destruction of the vertebral bodies can be seen in the radiographs in Figures 5 and 6. Figure 5 shows the collapse of the vertebrae inwards creating a wedged shape in the neck. Figure 6, taken through the open mouth of the patient in order to gain a clear veiw of the vertebral bodies of the cervical vertebrae in the neck, shows a loss in denisty and clearly defined outer edges of the vertebral bodies due to collapse.

It is likely the request for all bones in her body to be x-rayed came from the suspicion that other areas of the skeleton had been affected by the disease. The request was carried out with the x-ray report card indicating that anteroposterior (AP) and lateral radiographs, where possible, were taken of the chest, spine, legs and hips. The patient was immobilised on a Bradford frame, a rectangular metal frame with canvas straps to hold the individual in a prone or supine position, seen in the right hand image of Figure 4.
Between September and December 1948 the patient is noted to have developed a number of additional symptoms, including vomiting sputum; patchy erythema (a scarlet rash) on her chest; purulent nasopharyngeal discharge (discharging pus from the nose); aural discharge; an inflamed throat and enlarged cervical glands.
By July 1949, these symptoms had largely been addressed and the patient was showing improvement. Immobilisation was considered satisfactory as a form of treatment and a moulded plastic splint was to be prepared for the patient, to consist of
‘a jacket taken from the hips and extending upwards to embrace the head and the occipital region to the chin.’
This was later described as being reinforced with steel both vertically and transversely.
One year later, further examination by Mr Stanger noted that the disease had involved the 2nd, 3rd and 4th cervical vertebrae; the bodies of the 2nd and 3rd were showing signs of fusion and bone regeneration. It is at this point in July 1950, two years after first being admitted, that the child was allowed to ‘get up’.
This patient was discharged in December 1950, as being clinically and radiologically inactive and able to dispense with the splint. She continued to be seen as an outpatient at Stannington until 1956. Her last out-patient report stating that there was no deformity and no limitation of movement. Sound fusion was noted between both the vertebral bodies and posterior articulation of the 2nd, 3rd and 4th cervical vertebrae.
Further radiographic images can be seen on the Stannington Sanatorium ‘Radiographs from Stannington’ Flickr stream https://www.flickr.com/photos/99322319@N07/sets/72157648833066476/
Sources
Miller, F.J.W, Seal, R.M.E and Taylor, M.D (1963). Tuberculosis in Children. J & A Churchill Ltd.
Roberts, C and Buikstra, J (2003). The Bioarchaeology of Tuberculosis: A Global View on Reemerging Disease. Univesity Press of Florida.
Roberts, C and Manchester, K (2006). Archaeology of Disease (3rd Edition). Cornell University Press.