The radiographs held within the Stannington Sanatorium Collection date between 1936 and 1953 and are specific to the period when the sanatorium was used as a hospital for tuberculous children. However, through the process of listing the patient files for Stannington, which continue up until 1966, well into its use as a general children’s hospital, we have uncovered a set of radiographs for one other patient, a 6 year old boy who was admitted to Stannington on 15th June 1959: Patient 133/1959.
Patient 133/1959 was diagnosed with Fibrocystic Disease of the Pancreas, a generalised hereditary condition amongst children which, despite its name, can affect not only the pancreas but also the liver, lungs and sweat glands and was considered to be the most common cause of chronic non-tuberculous lung disease in children during the 1950s.
This patient was admitted to Stannington with widespread cystic change in both lungs, retarded growth and signs of chronically infected bronchiectasis. His medical notes also refer to ‘finger clubbing’, which involves changes to the areas of soft tissue under and surrounding the finger nails but may also involve the nails themselves. At this stage in his treatment the patient was prescribed penicillin, monitored for changes in weight and subjected to postural drainage.
By September 1959, the boy’s medical notes read:
‘No gain in weight and very little sputum but he has many loud râles in both sides of chest and a loose cough.’
At this time it is also noted that he has been prescribed pancreatin, a drug to help treat the symptoms of cystic fibrosis and to aid with digestion of fat, starch and protein. His lack of weight gain was considered to be associated with problems in the colon and as such his stools were also monitored regularly.
Little change is seen in the notes for the following year, weight gain is still elusive and the patient is often referred to as being small, with râles in the chest and having shortness of breath. However, in October 1960 the severity of this patient’s condition becomes clear as the attending physician writes:
‘Very poor appetite and very difficult.
I do not understand how this problem can be solved.’
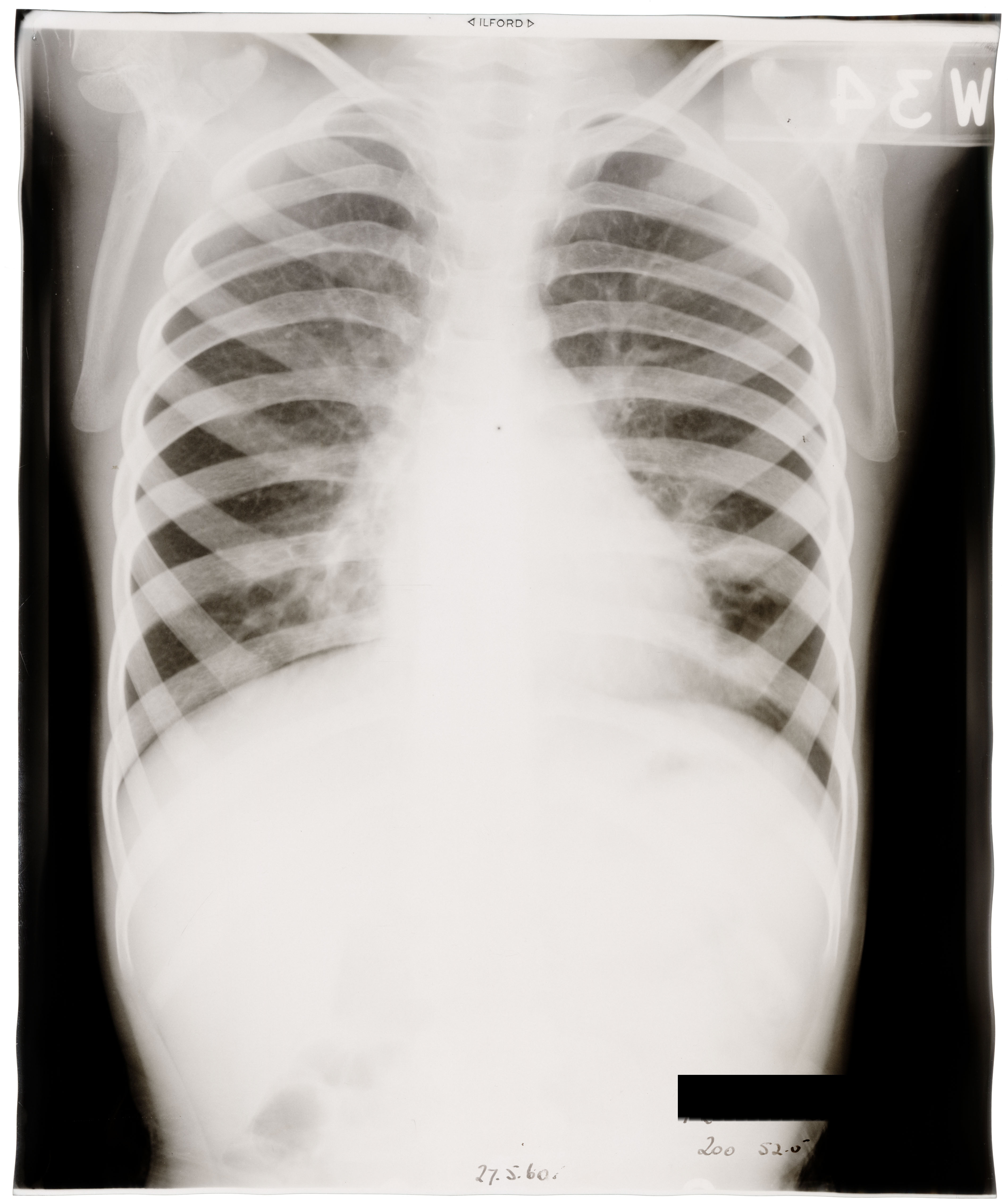
However, from May 1961, this boy began to show slow improvements especially within regards to the colon and weight gain is evident with a total gain of 8lbs since admittance. Râles are still noted in the left side of the chest, see lung x-ray in Figure 1.
In addition to his medical problems this boy also had learning difficulties according to notes from the hospital school teacher stating he was:
‘very much retarded and would need more individual help and attention ….
He is slow to complete written assignments but makes a good effort. His reading and arithmetic are well below average for his age but he has made satisfactory progress in both within his limited ability.’
As a result the doctors approached the subject of finding this boy a long term residential school for handicapped children to be transferred to following his discharge.
Patient 133/1959, remained in Stannington until 1962, where he continued to make improvements regarding his weight and height and the râles in his chest diminished significantly. In March 1962, he contracted German measles and then later chicken pox in June 1962. Despite these short term illnesses, this patient was discharged home in August 1962, having secured a place at the Windlestone Hall residential school near Ferryhill, County Durham, to begin in September 1962.
Sources:
di Sant’agnese, Paul. A (1955). The Pulmonary Manifestations of Fibrocystic Disease of the Pancreas. Chest. 27(6):654-667
Medline Plus (2015). Clubbing of the Fingers and Toes. http://www.nlm.nih.gov/medlineplus/ency/article/003282.htm
Patient (2015). Pancreatin. http://patient.info/medicine/pancreatin