Whilst the majority of the case files we hold are for patients who suffered from tuberculosis, a significant number of the latter case files we hold are not. In the middle part of the 20th Century detection and antibiotic treatment for T.B. developed and social conditions improved. This resulted in fewer children suffering from the disease requiring hospital treatment and beds being made available to children suffering from other complaints. From just a few non tuberculosis patients admitted in the mid-1950s numbers grew and in the 1960s around 80 in every hundred patients did not suffer from tuberculosis. Here we will look at the range of other illnesses and afflictions which children admitted to Stannington suffered from during this period.
To begin with, starting in 1956, non T.B. patients were admitted by referral from the same three visiting consultants who oversaw the treatment of tuberculosis patients. These patients were children who had chronic illnesses including asthma, respiratory infections, rheumatism and orthopedic conditions. This reflected the individual specialisms of the visiting consultants who were treating T.B. patients, and the illnesses it was thought would benefit from the environment and experience of the sanatorium and its staff.
By 1959 the situation had changed to the extent that most patients did not have tuberculosis; In the extract below from a letter found in a patient file, Dr Miller, one of the consultants who oversaw the care of patients at the hospital, explains what has changed.
Until a few years ago it [the sanatorium] was used entirely for children with tuberculosis, but recently as the number of children suffering from clinical tuberculosis has decreased so remarkably and social conditions have improved, we have been able to use the hospital for non – tuberculosis chronic respiratory disease and now the children with tuberculosis are in the minority.
From this point onwards the range of conditions which patients admitted to the hospital suffered from continued to grow. The table below summarises the range of conditions patients admitted to the hospital were diagnosed with in 1966, the last year of admissions for which we have case files, and is also illustrative of the preceding years in the decade.
| Diagnosis | Cases admitted in 1966 | % of total |
| Asthma | 36 | 23 |
| Tuberculosis (all types) | 21 | 14 |
| Behaviour Problem | 15 | 10 |
| Bronchitis | 13 | 8 |
| Chronic Respiratory infection | 9 | 6 |
| School Phobia | 7 | 5 |
| Bronchiectasis | 4 | 3 |
| Rheumatism | 4 | 3 |
| Diabetes | 4 | 3 |
| Muscular Dystrophy | 3 | 2 |
| Enuresis | 3 | 2 |
| Epilepsy | 3 | 2 |
| Malnutrition | 2 | 1 |
| Chorea | 2 | 1 |
| Eczema | 2 | 1 |
| Bronchopneumonia | 2 | 1 |
| Meningocele, glomerulonephritis, leg injuries, abdominal pain for investigation, endocarditis, headaches, osteitis of pubic ramus, Coeliac disease, Marfan’s syndrome, post pneumonia, neuroblastoma, Perthe’s disease, streptococcal infection, paralysis, obesity, for observation, habit spasms, post burns, fractured leg, scoliosis, mesenteric adenitis, post road accident, fibrocystic disease, pschomatic vomiting and amystonia congenita all accounted for 1 diagnosis on admission each. | 16 | |
The largest proportion of patients admitted to the hospital suffered from respiratory conditions such as asthma, bronchitis, and respiratory infections. Orthopaedic cases, conditions and injuries affecting bones and joints are also present. Patients diagnosed with psychological complaints make up a large group of patients admitted to the hospital. In addition to these there a number of other conditions are represented in the patient files; these include diabetes, obesity, chorea and admittance for a period of recovery after suffering from burns.
Patients suffering from asthma or other bronchial conditions were often admitted for several months or years at a time with the aim of improving their condition. For these patients treatment often included antibiotics such as penicillin, breathing exercises and postural drainage. If judged well enough, patients were often allowed home for holidays with permission from doctors. This allowed the patients to visit their families and also appears to have been used to trial patients in their home environment to see if they could sustain improvements in their health outside the hospital environment.
In the latter years of the time for which we have files patients were admitted with a range of psychological complaints. These were varied and include depression, psychosis, anxiety and school phobia. School Phobia, or the refusal to go to school, often had an underlying cause of depression or anxiety. These patients often came from difficult home backgrounds and were often admitted in part to give them respite from the home environment and the conditions which were causing their conditions. During the 1950s the care of these patients was overseen by Dr Connell, a consultant who had originally started visiting the hospital to see patients who had been admitted with conditions which it was felt may have in part had psychosomatic causes.
Children with orthopaedic conditions made up another group admitted to Stannington. Some of these were congenital, for example Perthe’s disease and talipes equinovarus (club foot), and some had other causes such as accidents. These patients were often admitted for recovery in a medically supervised environment following procedures and operations carried out at the general hospitals. The Royal Victoria Infirmary and Fleming Memorial Hospital in Newcastle feature regularly as places from which cases are referred.
In a large number of cases other factors played a role in a child’s admission alongside their medical condition. The continued provision of education meant that children were able to continue learning whilst their health improved. This appears to have been a particularly important factor in the cases of children with bronchial complaints such as asthma who outside Stannington could be missing large chunks of education. Schooling played such a large role in hospital life that admissions, discharges and holidays were commonly scheduled to coincide with school terms.
Home and social condition also played a role in the decision to admit children to Stannington. Examples include poor or overcrowded housing, a disrupted family environment, or where it was considered care or treatment administered by parents may be unreliable.
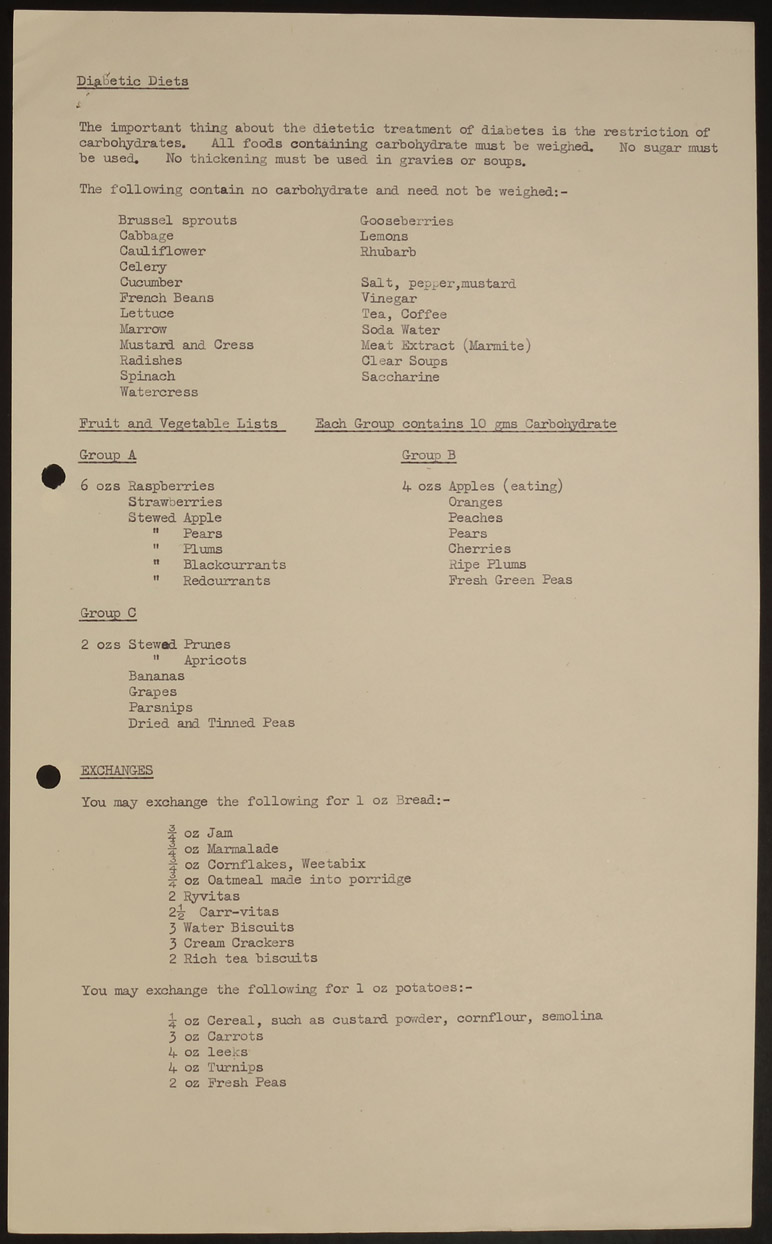
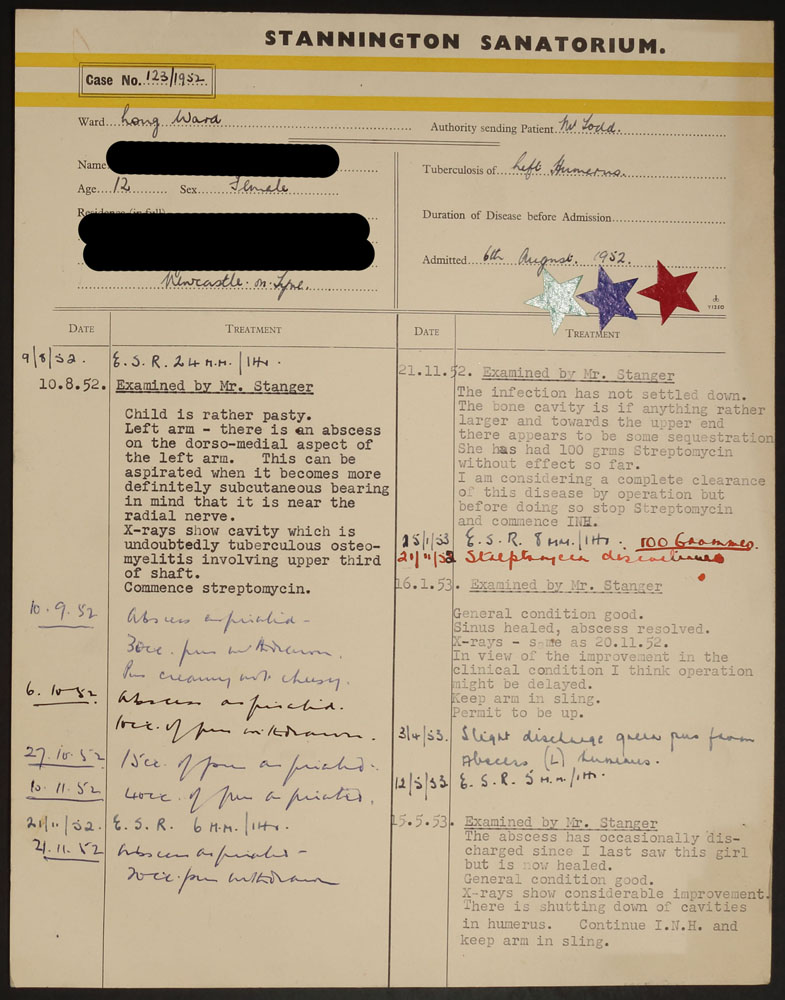
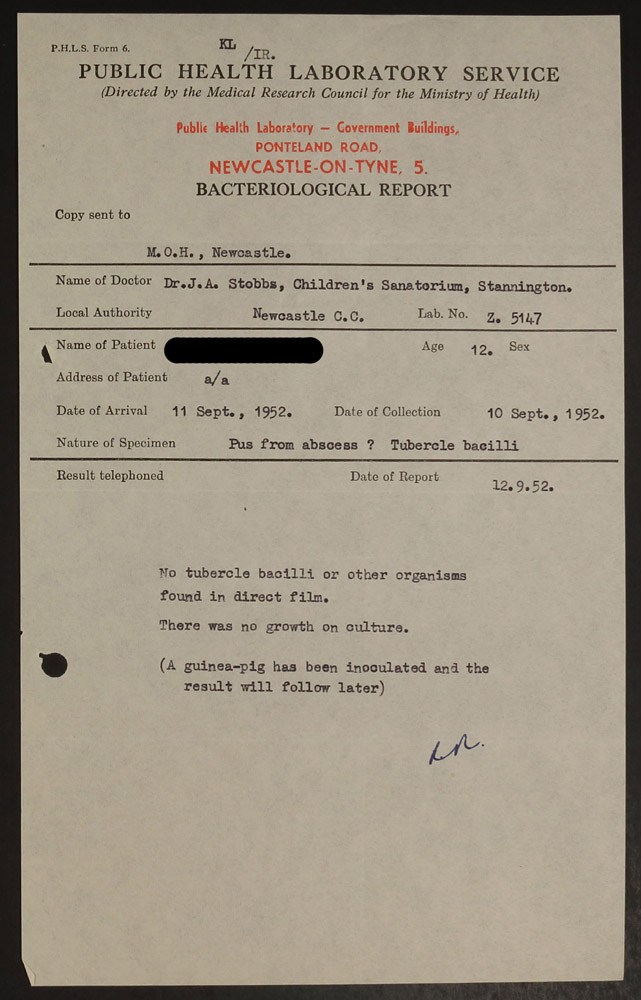
The case files for patients not suffering from T.B. largely follow the same format as that for T.B. patients. The case files for non-tuberculosis patients often include numerous letters regarding the progress of the patient’s recovery and arrangements for check-ups and procedures at other hospitals. These could often involve Stannington, the visiting consultant overseeing the patients care, specialists at other hospitals who were involved in a patient’s treatment, the family of the patient and the family doctor. In addition there can be other documents included in the files such as weight and height charts. One example is the page below, which is a dietary guide found in the file of a patient who was admitted to Stannington after being diagnosed with diabetes.