Daily life at Stannington didn’t just revolve around patients recovering from illness.

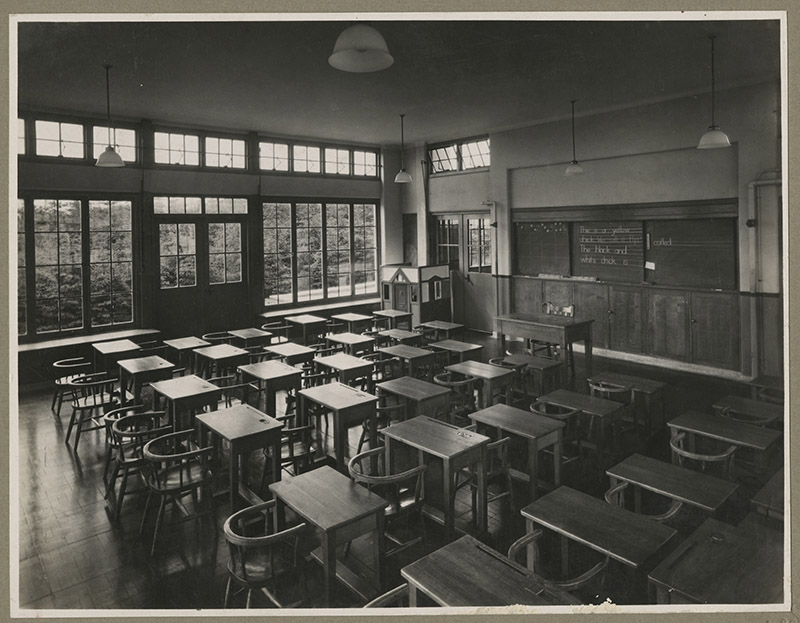
Education and time for recreational activities were also included in the daily lives of children staying in the hospital. As patients often stayed for many months or years at a time continuing education was considered so important the hospital had its own school. For part of its history the hospital also had a member of staff whose sole job was to look after the patient’s welfare and recreation needs.
In one of our patient files from 1966 we have found a daily schedule of activities. This illustrates how structured daily life was at the hospital.
As the daily timetable shows, the day started with postural drainage, breathing exercises or the taking of medicine, the exact nature of this varied with the patients and their complaint. After breakfast the school day began at 9.15. During a long lunch break children were again allocated time for treatment and a short period of free time. In addition, in the middle of the day, 45 minutes of bed rest was scheduled before the children returned to school for afternoon lessons.
At the end of the school day time was again allocated for treatments before tea time at 4:30. Visiting by relatives was allowed between 5.00 and 6.30pm. We know that this element of the child’s day did change over time. Until the mid-1950s visiting was only allowed on the 1st Saturday of each month meaning that children went long periods without seeing their parents; and other children including siblings and friends were not allowed to visit at all. Even in the 1960s its unlikely parents visited regularly during the evening due to the hospitals rural location and the wide geographical area from which patients were admitted. Bath time was between 6.30 and 7.30pm and bed time was set at 9.00pm.
During weekends and holidays without school to attend the children had much more free time but much of the other daily structure remained. On Sundays church services took place between 9.00 and 9.45 am, we know the hospital had its own chapel where these could take place.

To manage this time in its earlier days the hospital employed a Welfare and Recreation Officer who arranged activities for the children. In this role he reported to the Hospital House Committee which oversaw the daily workings of the hospital. Activities organised included handicrafts, walks around the grounds, billiards, table tennis and film shows.
In addition to regular film shows which took place during the winter months the hospital also had television in the wards, it is often noted in a patient’s care summary card when they were judged well enough to be allowed out of bed and watch television. These televisions were installed early in the 1950s, 5 were purchased by the hospital’s Coronation Celebrations Committee which was formed to arrange the celebrations to mark the queen’s coronation in 1953. The Stannington Scout and Guide Group Committee contributed £40 to this.
For the January 1954 meeting of the Hospital House Committee the Welfare and Recreation Officer reported on the range of activities in progress:
“Handicrafts The following handicrafts are still being done, rug making, stool making and seating, some plaster cast work, lampshade covering, leatherwork and embroidery.
Indoor Games Two billiard tables are always in full use and also the table tennis table, a new set of table tennis bats and a set of billiard and snooker balls have been purchased from a money allowance from the Sanatorium Scout and Guide Fund.
Film Shows Two film shows were held this month and the following films were shown – “Rock River Renegades”, “Thunder River Feud”, “No Indians Please” also a good selection of cartoons.” (HOSP/STAN/1/2/6)
In addition to the regular activities on occasions the hospital played host to touring Gang Shows and local pantomimes. The hospital’s League of Friends arranged day trips for the children and each year the hospital held a sports day and fancy dress parade. (You can read more about Sports day and the special event to mark the hospital’s golden jubilee here).
Outdoor activities for the children included going on walks around the grounds led by the Welfare and Recreation Officer, playing sports such as cricket and football on the hospital sports field and using the swings and roundabouts which the hospital also had. For a short time in the 1950s and 60s the hospital also had its own Scout, Guide, Cub and Brownie groups.

The children clearly made use of the facilities as now and again we see reports of accidents in patient files where children have been injured during these activities. For example in 1946 one child was hit in the right eye with a cricket bat (we presume accidentally!) and suffered bruising. Whilst practising on the morning of Sports Day in 1958 a child fell, put her arm through a plate glass window and suffered lacerations. On occasions accidents whilst playing resulted in broken bones and children had to be referred to general hospitals in Newcastle for orthopaedic treatment.
The daily activity timetable mentions that children were able to play with toys, games and jigsaws. These were often donated to the hospital by local groups, businesses and the hospital’s League of Friends and were listed by the Matron at the end of her monthly reports to the Hospital House Committee along with other gifts to the hospital.
Whilst this post has looked at what daily life was like in the 1950s and 60s children would have been occupied in many of the same ways throughout the hospital’s existence. Education always formed an important part of the daily routine for patients around which other activities were organised. You can read an earlier blog post about Mary Ann Fulcher who was headmistress of the Sanatorium for 30 years until her retirement in 1951 here.