Amongst the patients admitted to Stannington Sanatorium there are a number for which following admission doctors decide that their condition for whatever reason is non-tuberculous. Differential diagnoses can vary from bronchiectasis and asthma in those suspected of having pulmonary TB to Perthes’ Disease in those suspected of having TB of the hip. One patient who ultimately appears not to have TB is patient 90/38, a 17 ½ year old girl presenting with strong neurological symptoms, although no definite conclusions seem to be drawn on what the cause might be.
Admitted on 12 Sept 1941, she is one of the very few private patients and also one of the oldest. The diagnosis given at the top of her file is ‘Non-TB, query bone tumour spine and skull’. She had been suffering from symptoms for a year prior to admission and reports immediately following admission state ‘Lower thoracic curvature, no active angular deformity. Not tuberculous’.
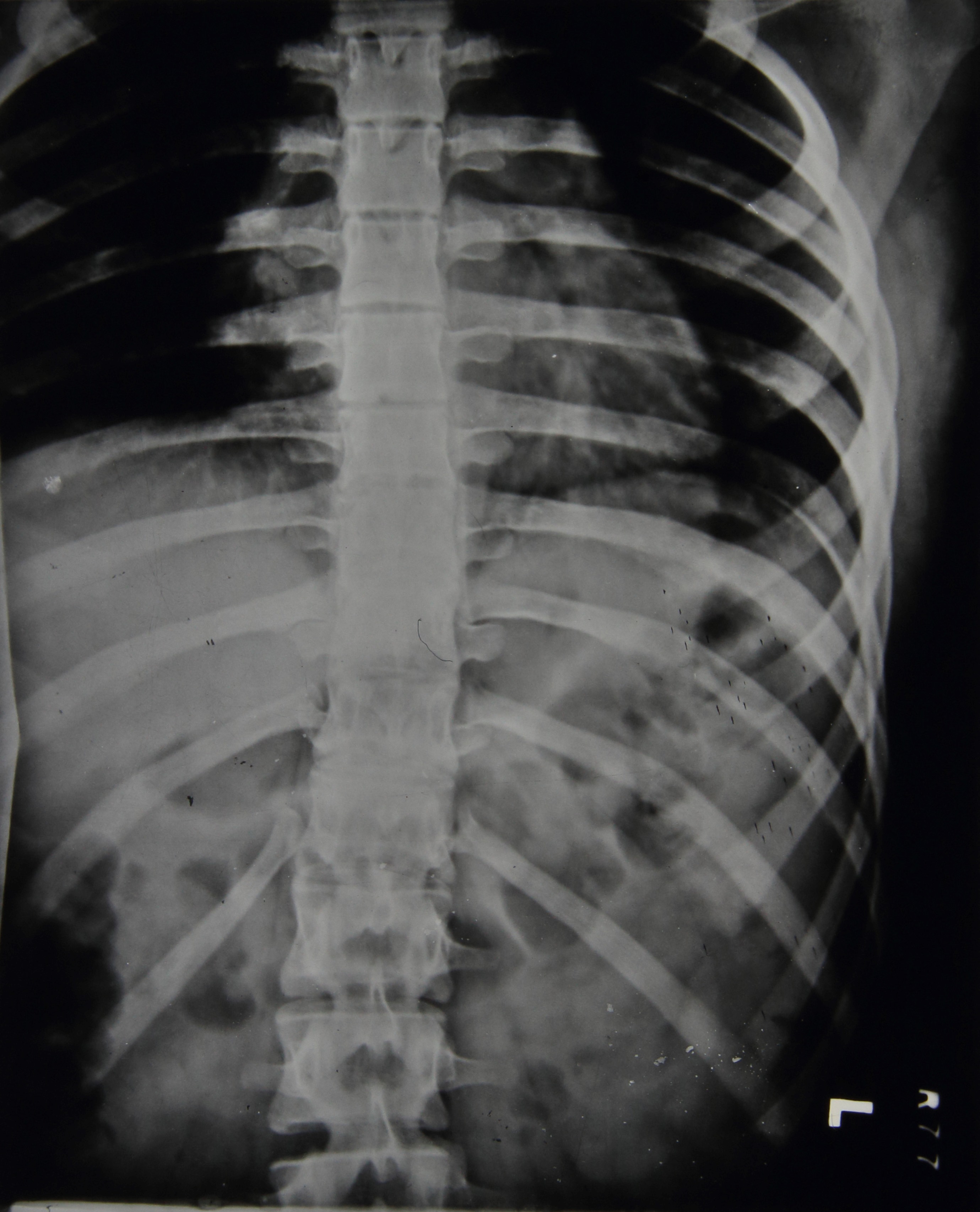
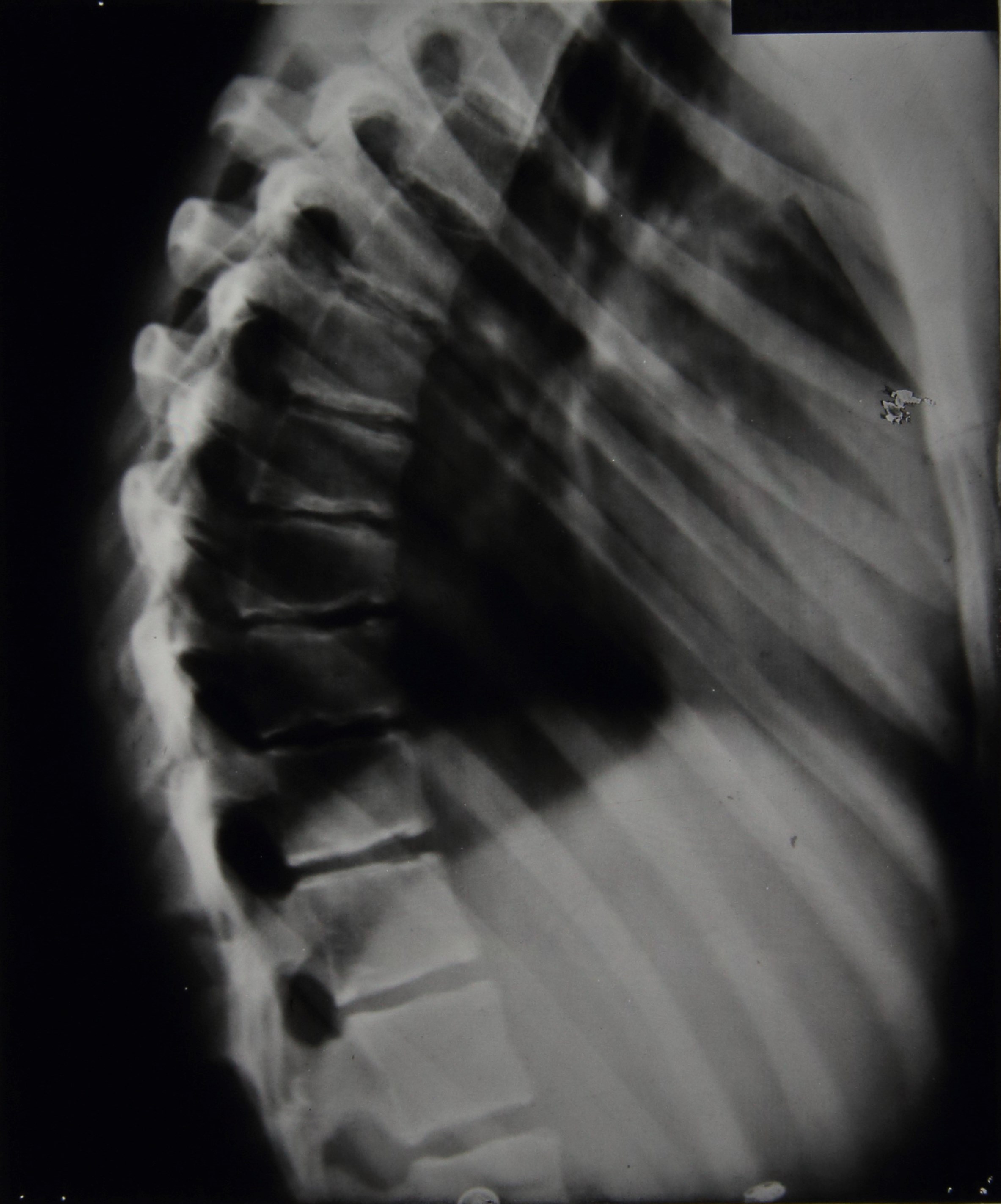
The first x-rays of her spine are taken the day after admission and here the report reads:
Marked irregularity of epiphyses in lower thoracic region. Some wedging of bodies of 9th and 10th dorsal vertebrae. Edges of bone are irregular & ossification is either incomplete or of poor quality.
Diagnosis: Epiphysitis of thoracic region, probably not tubercular
Over the coming months further spinal x-rays and their corresponding reports do not suggest any significant worsening of the spinal wedging nor any great improvements. The final report indicates that 5 vertebrae are affected with the 9th and 10th being the worst. Figures 1 and 2 are examples of some of the spinal x-rays that were taken.
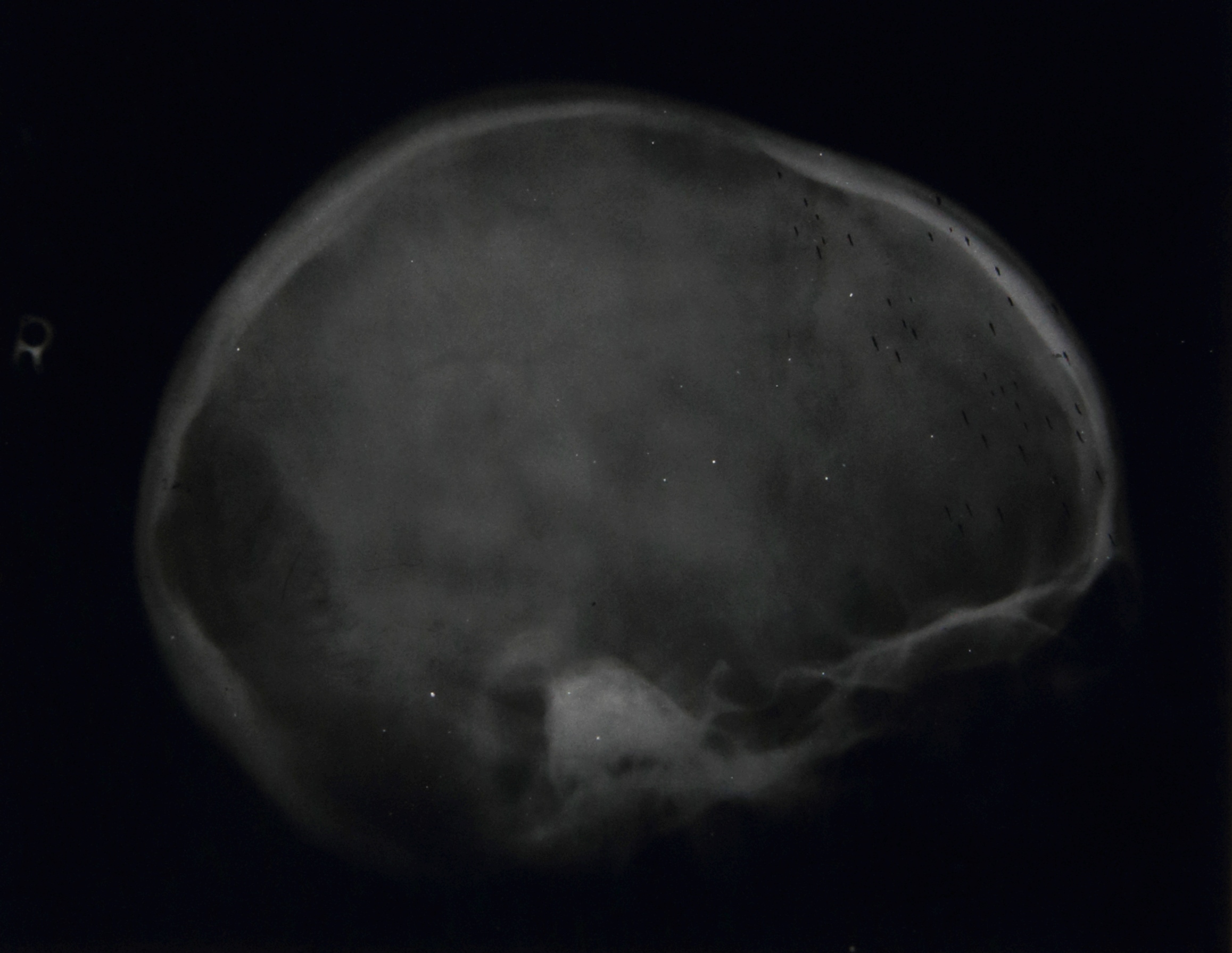
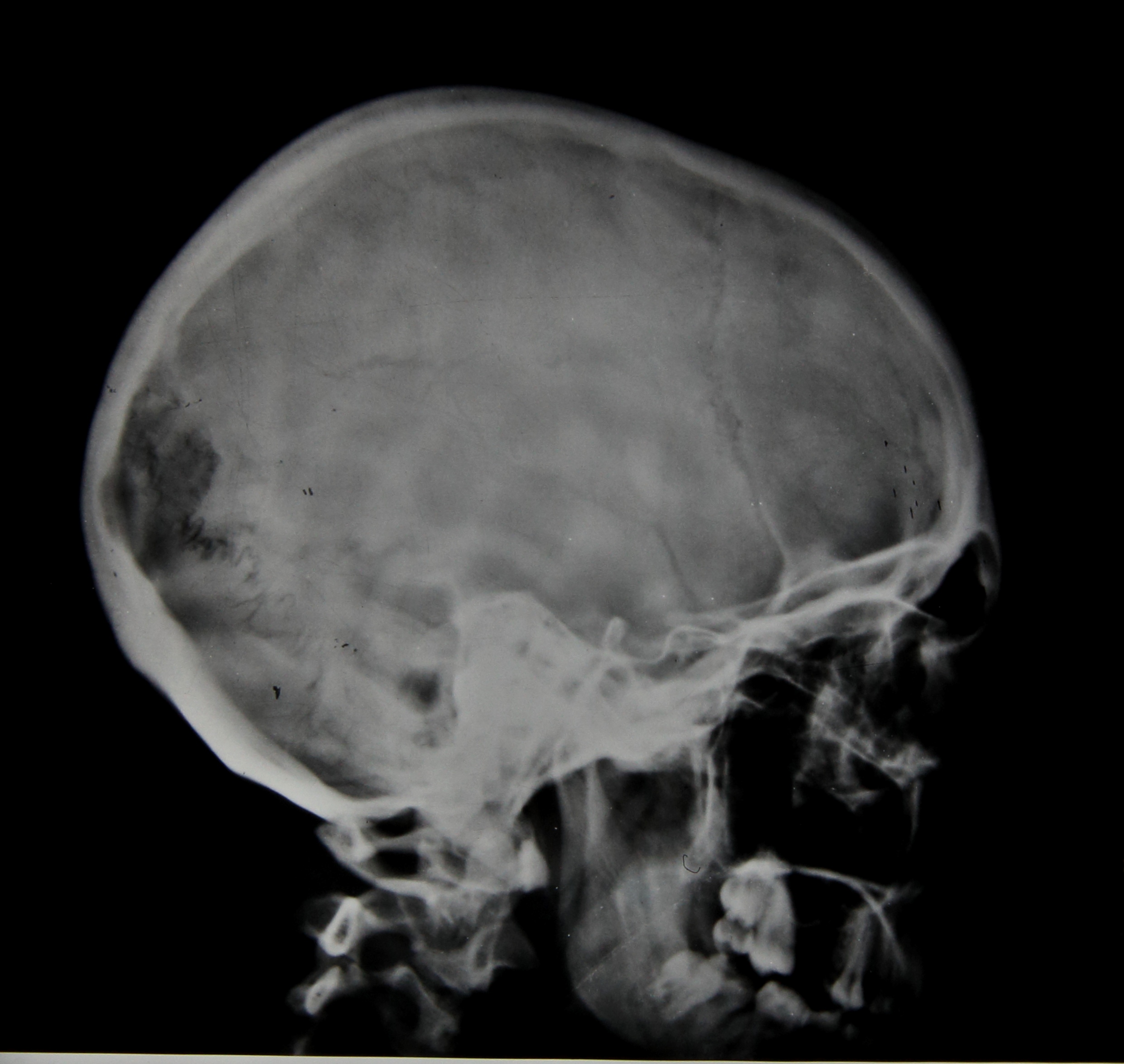
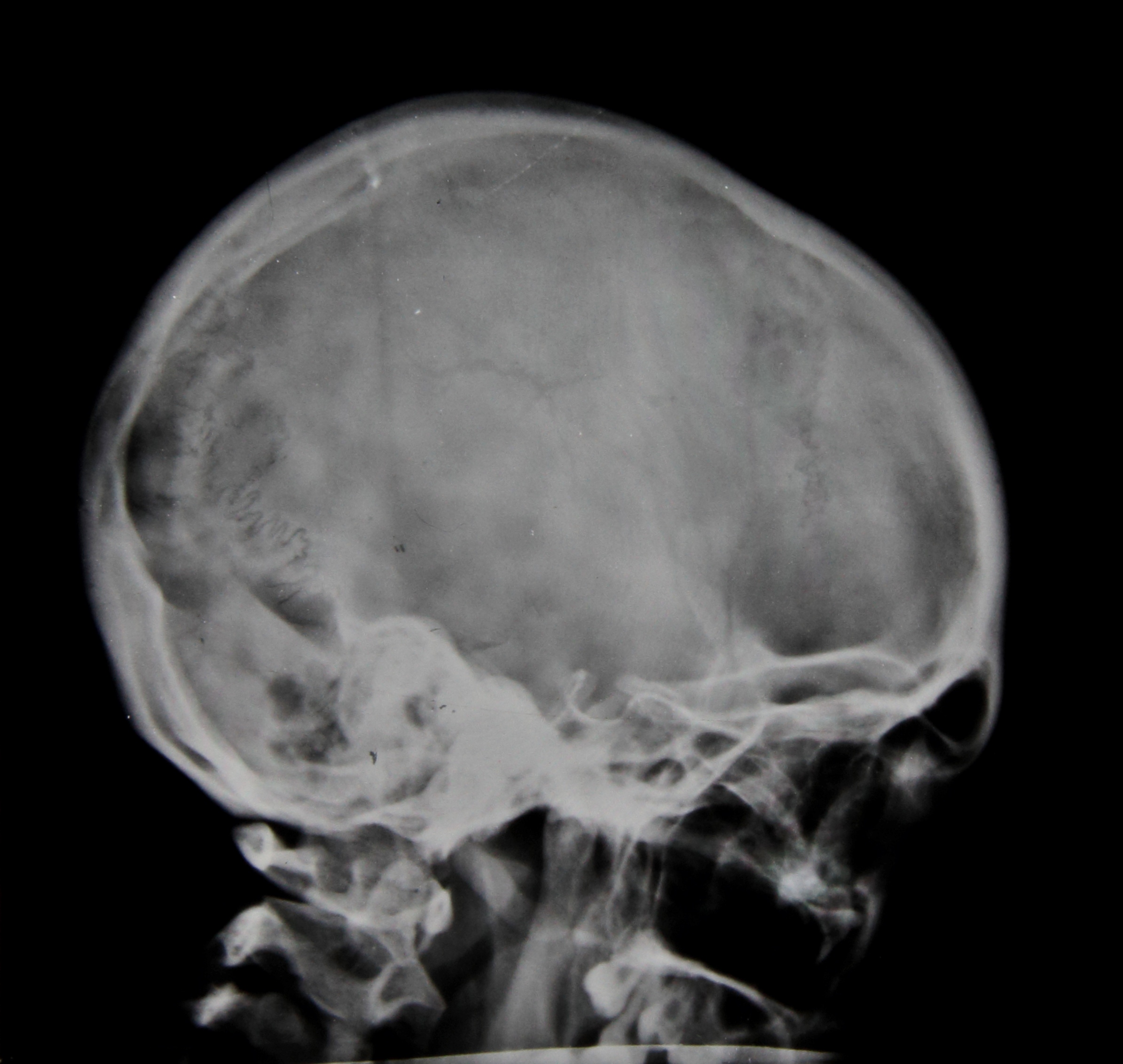
In addition, x-rays were taken of her arms, forearms, pelvis, femora, and legs, all of which were clear. There are also 7 x-rays taken of the skull, 4 of which can be seen in figures 3-6. Reports on the skull x-rays read as follows:
9/12/1941: Skull, localised deficiency of internal table to left of midline – lying over leg area.
19/3/1942: Outline of internal table broken for about 1” in anterior-parietal region.
14/5/1942: Rarefaction appears to be falling in. Outline more normal. Break still about 1”.

Her file also contains quite detailed reports on other tests carried out and her general condition during her stay. In November 1941 reports are made of signs of mental disturbance and that she ‘will not speak to anyone and only laughs or cries when spoken to’. She is also experiencing some incontinence and has a history of incontinence between the ages of 8 and 14. She has bilateral ankle clonus and a positive Babinski test, more marked on the right. Two days later the report reads as follows:
Spasticity lower limbs. KJs +. Bilateral ankle clonus. Plantar Reflex? – probably flexor. Sensation apparently normal. Pupils reacting normally. Eye movements, other cranial nerves & field of vision-apparently normal but patient unresponsive & difficult to examine.
She says she feels miserable & that everyone thinks she is silly, & that she has been like this before.
Still some incontinence.
At the end of November 1941 it is noted that there is a white patch in the centre of the optic discs and that the disc edges are blurred, still some spasticity, slight clonus, sluggish Babinski, normal co-ordination, normal mental condition, and occasionally experiences some frontal headaches. In March of 1942 a Wassermann Test comes back negative and she is eventually discharged on 16th May 1942.
If anyone can offer any further opinions on the possible causes of her condition please feel free to add your comments below.
Hi,
Recurrent meningitis is rare but usually associated with Streptococcus pneumonia, in this case maybe a secondary infection to the wedge fractures which may be caused by osteoporosis? (I know she is only 17 but, hey its a rare case!)
Cheers
Phil
I was wondering if it could possibly be Spinal Stenosis caused by some type of tumor/s that may explain some of the symptoms like wedging, problems with her mental faculty, incontinence. It’s normally seen in older individuals but can be seen in those with injuries/ tumors, and is more prevalent in females.
http://www.mayoclinic.org/diseases-conditions/spinal-stenosis/basics/definition/con-20036105
Amanda
Xray: spinal: destruction of anterior aspects of vertebral bodies of 2 lower thoracic vertebrae. The anterior aspects of end plates of 3 lower thoracic vertebre are deficient. There is wedge collapse of ?T6 and 7.
Diagnosis: ? Scheurmans disease ?tuberculous anterior and paradiscal destruction of 3 lower thoracic vertebral bodies, ?tuberculous wedge collapse of ?T6 and 7
XRay:cranium: Fig5. Erosive destruction of endocranial surface of occiput. Irregular radiolucent endocranial area at the site with ?reflected dura on to the internal surface of the radiolucent lesion. Irregularity of the inferior zone of the lesion.
Fig6. Radiolucency of the outer table with perilesional sclerosis.
Diagnosis: ?tuberculous diploic abscess with perforation of inner and outer table and endocranial extradural abscess.. ? Extradural (intra osseous) occipital meningioma.
Clinical observations of physical signs ofupper motor neurone lesions may be due to spinal stenosis at the site of the wedge collapse of vertebrae. The blurred optic disc margins indicate probable raised intracranial pressure.
Langerhans cell histicytosis can cause osteolytic lesions in the skull, mandible, vertebrae and long bones
Bes wishes
Eduardo F. Moya
Consultant Paediatrician
Bradford Teaching Hospitals